In this third and last post on cholesterol and Coronary Artery Disease (CAD) we will talk about what you can do to lower your risk. In the first post we broke down the myths of the Lipid Hypothesis (located HERE) and in the second we covered what really causes Coronary Artery Disease (CAD) (located HERE).As I eluded to in the first post, CAD is primarily caused by oxidative damage and inflammation. The 4 primary causes of oxidative damage and inflammation are:
- Poor Nutrition
- Stress
- Smoking
- Physical Inactivity
Let’s break each these factors down.
Smoking
So we all know we shouldn’t smoke. Smoking as few as 1-4 cigarettes a day increases your CAD risk by 40%. 40 a day increases risk by 900%!! I don’t think I need to say much more on that one.
Physical Inactivity
We also know that being physically active is important. People that are not physically active have 1.5x to 2.4x the risk for heart disease. Currently more than 60% of Americans are not regularly active and 25% are completely sendentary. Regular excessive reduced both inflammation and oxidative damage. There are many ways to increase your physical activity. It doesn’t mean you have to go to them gym and run on a treadmill. Just going to the grocery store, parking at the far end of the lot, shopping for your food and coming home to cook a meal instead of going through the drive through can make a difference. Walk around the block and increase from there. Walk the dog. There are a lot of activities that we can do to increase our excessive and reduce our risk of heart disease.
Stress
Stress is important to keep low as this can be a big contributor to CAD risk. This Study showed that stress can triple the risk of heart disease. This is when we get that “fight-or-flight” response that we experience when under high stress. This elevates cortisol which causes both oxidative damage and inflammation. A great way to reduce stress and increase physical activity is with something like Yoga!
Poor Nutrition
The best thing you can do to influence your risk of CAD is through diet. This study of 52 countries found that 90% of heart attacks could have been prevented through diet. That’s right, 9 out of 10 heart attacks could be prevented without drugs. So what foods cause oxidative damage and inflammation? There are several sources and we will break down the biggest ones. This biggest contributors to oxidative damage and inflammation are sugar (sucrose, fructose, etc), starch (grains, etc), polyunsaturated (PUFA) oils and trans fatty acids (transfat).
Sugar!
One of the best studies on sugar consumption and how it relates to cholesterol levels is the 2011 study by Peter Havel and colleagues titled Consumption of fructose and HFCS increases postprandial triglycerides, LDL-C, and apoB in young men and women. In this study they had 3 groups in a randomized trail and had them consume the Standard American Diet (SAD) (55% carbs, 15% protein, 30% fat) with the difference being where the carbs came from in each group.Group 1: 25% of their total energy from glucose (so traditional sources, sort of the SAD control group)
Group 2: 25% of their total energy from fructose
Group 3: 25% of their total energy from High Fructose Corn Syrup (HFCS) (55% fructose and 45% glucose)This 25% of their diet coming from sugar equals about 120 pounds of sugar per year. That may sound like a lot, but that is actually below the current average for Americans. This figure shows the differences in LDL-C, non-HDL-C, apoB, and apoB/apoA-I.
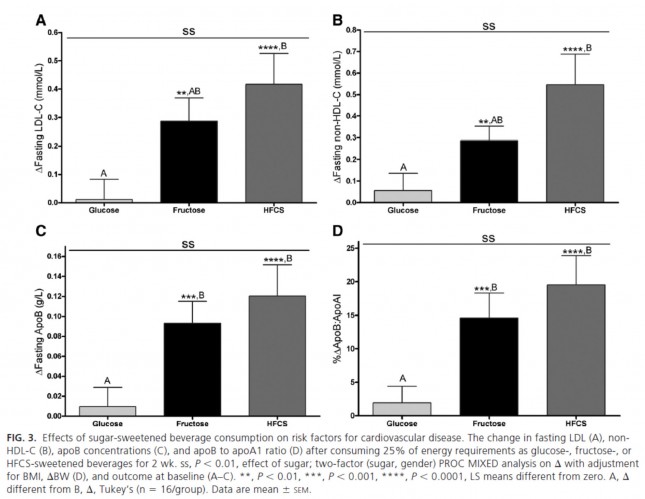
This is a very powerful indication that while glucose and fructose alone can be bad in excess, their combination seems even worse. It would have been really interesting to have an additional group that removed most carbs all together. (more on this in the carb section below)
Sugar and fructose are very inflammatory and cause lots of oxidative damage. What happens is when we consume large amounts of sugar and fructose, our insulin levels go up and it is this rise in insulin that causes tears in the artery wall. Cholesterol comes to repair this oxidative damage and build up causing plaque build up (as described Here in part 2). So it is imperative to keep our blood sugar levels (and thus insulin levels) balanced so that we don’t cause this inflammation and oxidative damage. So keeping sugar and starch low in our diets (to keep our blood sugars balanced) becomes the best way we can change our diet to reduce our chances of getting CAD.
Also important to note, as I did in This post, non-alcoholic fatty liver disease and metabolic syndrome are very big factors in CAD risk (as much as 14 times in women). So what causes non-alcoholic fatty liver disease? There is growing evidence that fructose consumption (fruits, fruit juices, etc) are a big contributor as well as high fructose corn syrup (source and source). When you consume fructose 100% of the metabolic burden rests on your liver. Only your liver can break it down. Glucose is only 20% broken down by the liver and the remaining 80% is immediately metabolized and used by the cells in your body. When fructose is converted into fat, it gets stored in your liver and other tissues as body fat. 120 calories of fructose is stored as 40 calories of fat in your body. 120 calories of glucose gets stored as less than 1 calorie in your fat stores. Fructose metabolism is very similar to alcohol making it one of the biggest contributors to non-alcoholic fatty liver disease.
Fructose also worsens insulin resistance which speed metabolic syndrome. This is a good video with more info on sugar.
Carbs
There is a great study by Jeff Volek that looks at the results of a carbohydrate-restricted, high-fat diet compared to a low-fat high carb diet and the results on cholesterol (source).
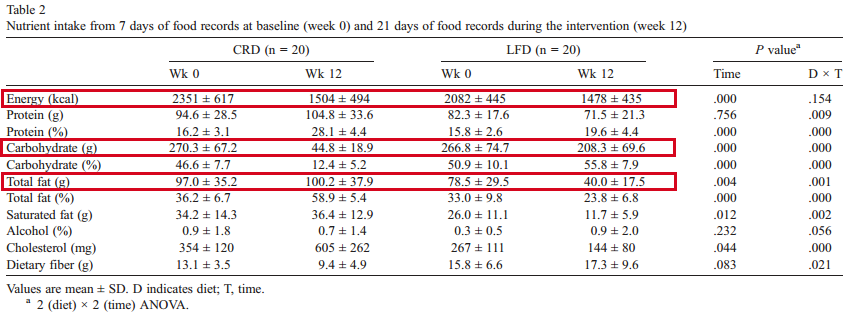
The two groups in the study were taken from a SAD diet to a carb-restricted diet (CRD or Very Low Carb, High fat diet) and low-fat diet (LFD or Very Low Fat, High Carb diet). As you can see the high-fat diet was mostly fat (100g or 900 calories) and very little carbs (44g or 176 calories). Here are the results after 12 weeks on each diet.
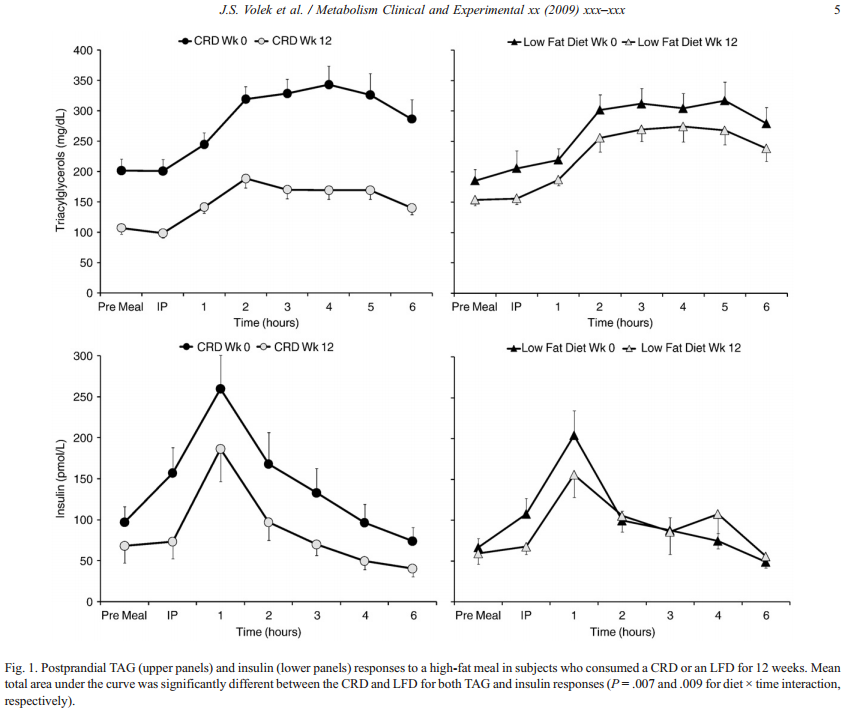
As you can see the Low Carb/High Fat diet reduced Triglycerides significantly and also reduced insulin levels greatly. The Low-Fat diet had statistically insignificant changes in both triglycerides and insulin levels. As we discussed in the last post, LDL particle number is the best predictor of CAD risk, but other measurements like Triglycerides can be indicative of issues that can contribute to high LDL-P. It is good to keep your fasting Triglycerides below 88.
Good Fats
This is the component you want to increase the most (while decreasing carbohydrates) to help protect against heart disease. Especially important are saturated fatty acids (SFAs). Saturated fats like coconut oil, butter, ghee, tallow, and lard are protective against oxidation and inflammation and have many other important health benefits. I will have a post on fats coming soon to expand on this topic in greater detail. Studies like this one published in the Journal of Nutrition 2004 showed that saturated fat from MCT oil (medium-chain fats similar to those in coconut oil) and beef tallow reduced alcohol-induced liver damage when substituted for polyunsaturated corn oil. In fact, they replaced 20 percent, 45 percent, or two-thirds of the corn oil with saturated fat and found that the more saturated fat they used, the greater the protective effect. So saturated fat can be protective against one of this biggest risk factors for CAD, fatty liver disease. Here is another recent study showing the protective affects of coconut oil. There are several good oils that can be very helpful in reducing your CAD risk. Also, the higher the saturated fat content the better. Here are the best oils:
- Coconut oil: 1.9% PUFA (92% saturated fatty acids (SFA)
- Palm kernel oil 2% PUFA, (82% SFA)
- Cocoa Butter: 3% PUFA (60% SFA)
- Beef Tallow: 3.1% PUFA (49.8% SFA)
- Ghee: 4% PUFA (48% SFA)
- Butter: 3.4% PUFA (50% SFA)
- High Oleic Sunflower oil (9% PUFA)
- Macadamia oil: 10% PUFA (15% SFA)
- Avocado oil: 10% PUFA (11% SFA)
- Lard: 12% PUFA (with 41% SFA)
- Duck fat: 13% PUFA (with 25% SFA)
- Hazelnut Oil: 14% PUFA (with 10% SFA)
- Almond oil: 17% PUFA (with 8.2% SFA)
- Olive oil: 9.9% PUFA (with 14% saturated fat) (although this one should never be used for cooking which will cause oxidation. So only use in dressings, etc.)
So we should be consuming lots of these oils in order to reduce our CAD risk (as well as a huge number of other health benefits). Many studies have shown that the higher the saturated fat intake in the diet leads to less fat in the bloodstream (source). Where as the same study showed that low fat diets where carbs were high, had higher fat in the bloodstream.
Bad Fats
There are two kinds of fats that should be avoided. The most inflammatory fat is Trans Fatty Acids (transfat). Transfats are one of the worst substances we can consume for our overall health. There are many studies that show the heart disease and cancer risks of transfat (source, source, and many more for cancer, source, and source). Even the FDA has stated that “Further reducing trans fat consumption by avoiding artificial trans fat could prevent 10,000-20,000 heart attacks and 3,000-7,000 coronary heart disease deaths each year in the U.S.” Here is a list of transfats to avoid:
- Margarine
- Vegetable Shortening
- Ingredients that list Hydrogenated (fully or partially) Oils
Poly Unsaturated Fatty Acids (PUFA’s) are also bad oils as they are easily oxidated. This means they are very susceptible to oxidative damage, the thing that increases our CAD risk. There are many PUFA oils and here is a short list:
- Grapeseed oil: 70.6% PUFA
- Sunflower oil: 68% PUFA
- Flax oil: 66% PUFA
- Safflower oil: 65% PUFA
- Corn oil: 54.6% PUFA
- Walnut oil: 53.9% PUFA
- Cottonseed oil: 52.4% PUFA
- Vegetable oil (soybean oil): 51.4% PUFA
- Sesame oil: 42% PUFA
- Peanut oil: 33.4% PUFA
- Canola oil: 19% PUFA
What has happened over the last 100 years is a huge increase in PUFA consumption and a reduction in other good fats (like saturated fat). Here is a chart showing the increase in PUFA consumption in the US.
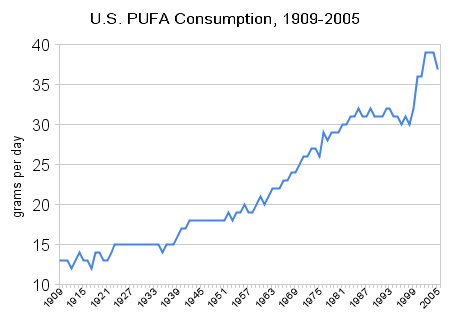
It is my belief that this is a big contributor to our increase in heart disease. So it is imperative to reverse this trend if we want to reduce the incidence of heart disease.
Note: PUFAs are essential fatty acids, so we do need them in our diet. When it comes to PUFAs, the type and how you handle them is very important. When using PUFAs, try to use them without heating too much (salad dressings, etc) to keep them from being oxidized and store them in the refrigeration to keep them from getting rancid (omega-3s like fish oil, flax, etc). The ratio of Omega-3s to Omega-6s should be closer to 1-to-1, but today many people eat a 1-to-20 or even 1-to-50 ratio of Omega-3s to Omega-6s. Omega-6s are also inflammatory when consuming too many and Omega-3s are anti-inflammatory. So it is important to make dietary fat intake from more saturated fats and less PUFAs and make the PUFAs we do eat a ratio closer to 1-to-1 of Omega-3s to Omega-6s. (Lots more about this Here)
Summary
There are many things you can do to reduce your risk of coronary artery disease (CAD). Some of these are obvious (quit smoking, reduce stress, increase physical activity). But nutrition can be the largest factor (preventing as much as 90% of heart attacks). The biggest nutritional contributor to CAD risk is sugar. High fructose corn syrup and fructose are particularly bad but all sugars will contribute and should be eliminated as much as possible. Other starchy foods also contribute to oxidative damage and inflammation so keep starchy food consumption as low as possible also helps CAD risk. Lastly, the good fats (saturated fats, coconut oil, MCT oil, ghee, butter, tallow, and cocoa butter) are very protective against oxidative damage and inflammation and should be consumed in high quantities in order to reduce your risk of CAD. The bad fats are the transfats should be completely avoided. PUFA’s should be limited and kept at a 1-to-1 ratio with Saturated fats or less. Eating lots of good fats, moderate amounts of protein and very low carbs (especially sugars) are the best ways to reduce your CAD risk. In addition, supplementing with CoQ10 can help decrease oxidation and improve heart health.











I’m wondering where Almonds and almond oil fit in here. Since the low carb diet so often depends on almond flour as a substitute isn’t that adding significantly to the Omega 6 intake and isn’t it also a PUFA?
Almond oil is on the list above. With 17% PUFA I see it as a good option if not going above it’s smoke point (and thus oxidizing it as with any oil).
If it’s 17% good stuff, then does it follow that it’s 83% not-so-good stuff? If not, then what is the rest of it made of?
Nope, that is 17% bad stuff. The PUFA’s are what you want to avoid. 🙂
Thank you, Im so careful now about everything that is not for your best interest.
Maria:
This isn’t directly on-topic, but I wanted to tell a bit of a story. I was diagnosed with Type II diabetes. Now, I grew up with a Type I diabetic brother so, as I said to my Family Practice doctor, “Now I have to eat like I always knew I was supposed to eat.”
Here’s the thing. I got this way eating relatively “good” food. I am a fairly serious cook, and I never ate truly “garbage” foods, but my weakness was (and still is) baking and baked goods.
Well, as you know, many of those foods went right out the window. Although it would be theoretically okay to have a slice of homemade white bread, I’m afraid that if a loaf of homemade white bread comes out of my oven, I’m eating at least half that loaf while it is warm.
It wasn’t un-liveable, putting aside baked goods, rice, potatoes, and other starch and sugar heavy foods. And I started playing around on my own with xylitol and lower glycemic starches and so on; producing pretty palatable baked goods that were about 1/2 the GL of regular, but still they were rare treats and I still had the “how do you eat just one” problem. The only thing I think I arrived at on my own as a “perfect” substitute was a sugar free, almond meal crust cheesecake that was indistinguishable from the bad version.
Then somehow I stumbled on your “Art of Eating Healthy: Sweets.” Finding tasty recipes with NO grain flours was one thing, but also finding things I had not heard of before (Just Like Sugar) and finding ways to use various nut flours that WORK, and finding ways to use whey and egg proteins as replacements for the role starches and sugars play in baked goods, well, I was THRILLED.
I’ve bought most of your other books as well now, and I recommend them to many people. I find my personal experience is that about half the baked goods “work” for me, and that’s a better ratio than many “regular” cookbooks. And in a couple of cases I like your recipes better than their original “bad” versions.
I have used my glucose meter to test the “validity” of many of your recipes and they are all great choices for diabetics.
NOW, all this said, I have found some things I would like to improve.
I know volumetric measures are traditional, but I find that with some nut flours, especially almond, but also peanut and coconut, you can get the same weight into 1 cup or 3/4 cup depending on how much pressure you use, and this has a definite effect on the final product. I would love to see everyone (not just you!) use weight measures (ideally in grams), even if you also provide volumes. Failing this, it would be good to know if it should be “packed,” “loose,” or “aerated.” It really does help.
One of my favorite recipes of yours is your almond meal/whey protein/psyllium husk powder pizza crust. LOVE it! But there I was thrown by “psyllium husk POWDER.” I found whole psyllium husks at the store and, of course, my first several crusts were VERY wet and hard to manage. This was my fault, not the recipe, but I made the mistake because of the relatively unfamiliar ingredients and not knowing that there was a distinct “powder.” (I food processed my whole husks, and found a place to order powder), but more “technique guidance” can help.
Finally, one more just outright praise: I have used your cauliflower “potato soup” to convince people who hate cauliflower that they now love cauliflower.
No matter what, your work is in the top five influences on my cooking, and you are the number one influence on my path away from metabolically destructive cooking. You may have singlehandedly made the difference in my diabetes control, and that means I might live ten or twenty years longer thanks to you. So weight measures really aren’t THAT important! 😉
I look forward to new recipes in your emails. Now I’m off to try your healthified snickerdoodle recipe from a week or so ago…
Thank you Michael! I appreciate the support and referrals. 🙂
This has been a very interesting series, Thank You. I am currently having “Discussions” with my Dr. about cholesterol, and more importantly about statins. He spouts the party line, but is willing to be educated (and, in fact, told me to eat “as few carbs as possible” when diagnosing me with Type 2, and discouraged me from going to the ADA nutrition class at a local hospital). And when he says my LDL is high, I ask him how he knows, since the equation they use to find that number breaks down if your triglycerides are below 100, which mine are.
On another note, I would like to second Michael’s request for weight measures (preferably in grams, for ease of multiplying or dividing) for ingredients. Especially for baking, but also sometimes for savory (for example, 1 cup chopped zucchini – how big is each piece?). You can get a perfectly good electronic scale these days for $35 – $45, which will switch between grams and pounds/ounces, and it really does make a difference in some recipes.
I must say, though I was a bit distressed to see the PUFA content of grapeseed oil. I just picked up a can of this, and was hoping it might be good for homemade mayo, but I guess it will not become my light oil of choice. I think I’ll try macadamia or avocado for the mayo. Thanks for all you do to educate us; trying to find honest evaluations of what is healthy and what not, especially for someone with a compromised metabolism, is a real challenge, and I do appreciate the work that goes into it. Kudos to you for doing it.
Thank you! 🙂
A few points…
Agree about using actual weight measurements, rather than volume. I’m used to using g and kg for baking. Cups throw me. I feel it’s a bit too close to ‘guessing’ for my fanatical-to-the-very-gramme cooking. 😉
Back in 1997, a Harvard-led study looked at the ratio of triglycerides and HDL with regard to the risk of a heart attack. Below 2 – low risk. 4 – high. 6 and over – high risk. “High triglycerides alone increased the risk of heart attack nearly three-fold.”
Yet we still get doctors only looking at LDL!!! Or just total cholesterol!!
(Citation: The ratio of triglycerides to HDL was the strongest predictor of a heart attack, even more accurate than the LDL/HDL ratio (Circulation 1997;96:2520-2525))
PUFA. Excellent acronym! Albeit accidental.
Finally, thanks for this superb analysis of cholesterol and CAD. If only the average doctor had this information!
Thanks! The triglyceride number is an important factor, but LDL-P is still the most predictive of risk (when you remove all other factors). Pete Attia does a much better job of explaining this in detail here (also lots of good stuff in the comments and the other posts in his series). 🙂
http://eatingacademy.com/cholesterol-2/the-straight-dope-on-cholesterol-part-ix
In the comments he addresses the issue of ratios and TG. Peter Attia “Ratios provide guidance, but should not be used for treatment. We treat LDL-P, but often the ratio of LDL-P to HDL-P or TG to HDL-C or ApoB to ApoA1 serve as quick checks of where you’d want to be (ideally, below 30, 1.0, and 0.34, respectively).”
Alas, the doctors through my employer only test for HDL, LDL (calculated) and total cholesterol. And I haven’t found an outside lab that does LDL-P – yet, but I’m looking. I refuse to be tested though the work doctors as they won’t get the right data and, going on the limited data they do get (in fact no matter what the numbers are), they will automatically prescribe statins. These are doctors who still talk about low fat diets and eating “healthy whole grains”.
Sorry that should be a lab I can walk into.
There should be some places out there that do it. They recently approved a smaller machine that can be used regionally so they should become more common. Here is one place. I have heard there are some that do it for less (under $100). 🙂
https://www.directlabs.com/Resources/Cardiovascular/NMRLipoProfile.aspx
I can’t stand the taste of coconut…Are there coconut oils without coconut flavor? Do the MCT supplements have the same benefits as the straight coconut oil? I use all the other oils…I have all your books…love them…
Yes, this one doesn’t have any coconut taste. The MCT oils are basically the saturated fat from coconut oil. Coconut oil has added benefits. 🙂
http://secure.ttpurchase.com/6D7F3919-1E0B-90B3-0E53DEB1424EA0A7
Thanks!
Ordered it…thank you. you should add that to your amazon store list…how do you cook/use, or do you use, cocoa butter with your family? I think you should write another book about healthy eating on the go and/or for portable lunches….exclusively recipes that need no or little refrigeration and can be eaten at work easily or at soccer games, etc. An expansion of the lunchables idea in the kids one. this is the last area I struggle with — lunches for husband and work that he can easily eat and that he likes….he loves HOT POCKETS…ouch…hate to admit that. that is the only thing bad in my house..
Thanks! I have a post that will go over healthy eating for families on the go or on vacation. I have lots of recipes that can easily be frozen and popped in a bag (mini quiches, muffins, etc). By the time it is lunch they are thawed. 🙂 Also, anything made with coconut oil will last longer without refrigeration. I have lots of ideas in my kids cookbook. 🙂
http://www.amazon.com/The-Art-Healthy-Eating-Kids/dp/0988512432/ref=sr_1_3?ie=UTF8&m=A51JBC26TWGDE&qid=1366988409&s=generic&sr=1-3
What neutral tasting oil do you recommend for lightly frying things like chicken or veal cutlets? I always thought 100% extra virgin olive oil was the best for everything until I learned differently. Then I thought grapeseed oil was a good alternative but I see here on the list that it is a no-no. And what does PUFA stand for?
There are a few options, depending on the flavor profile. We use beef tallow (what McDonalds used to use before they switched to the “Healthier” vegetable oils), expeller pressed coconut oil (doesn’t have coconut flavor) or leaf lard. 🙂
What is “leaf lard?”
Lard made from pig fat. 🙂
hi there maria, I have been removing all my estrogen producing and toxic skin care and household cleaner products, laundry etc. from my home and replacing with healthy altrnatives, even some homemade laundry soap recipes. I know that safflower oil and sunflower oils are polyunsaturated fats, unstable and not good for cad risk. this might be a silly question. but since our skin is so absorbant as you have taught us, it would seem that using skin care products that contain those oils is not a good idea. am I on the right track with this thinking? any thoughts on that question of mine?
I would be less worried about them there. You aren’t getting much of it into your system like you would ingesting it. 😉
thank you maria for your patience…;)
In your book Secrets to a Healthy metabolism, there is a list of dietary sources for healthy fats that include walnut (bottled oil), but I’m reading here that is high in PUFA… so I’m a bit confused… what am I reading wrong?
This list is more up to date. We are always learning new things with our research and try to keep everything up to date with the healthiest options. That book was written about 8 years ago so this info is more up to date. 🙂
Maria, I was wondering if you could recommend a quality olive oil? I have learned that many olive oils are cut in with other oils and that they oxidize when stored in glass bottles. is there an olive oil that you could recommend and is there anything else I can look for to know its quality?
It can be tough. I think this one is an ok option. 🙂
http://astore.amazon.com/marisnutran05-20?node=9&page=4
Hi Craig,
Thank you so much for writing these posts on Cholesterol! I read all 3 of them, but am still about confused about my levels… (I bought Maria’s full 90 day meal package, but – due to my chronic illness – have not been able to read most of the books, so if there’s an answer to my question there, have not been able to find it.) In any case, I have been eating “Maria’s way” for almost a year now, and my Cholesterol levels were just measured.
*Cholesterin (which apparently translates to simply “cholesterol”) = 312 mg/dl (normal range 50-200)
*HDL – Cholesteral = 107 mg/dl (normal range 50-200)
*LDL – Cholesteral = 191.40 mg/dl (normal 67-173)
Triglyceride (fasting) = 68 mg/dl (normal 30-170)
Chol.HDL-Chol-Quot. = 2.92 (normal 0-4.5)
LDL/HDL = 1.79 (normal 0-3.0)
The *s mark what the lab thought was abnormal. My doctor wants me on Statins due to the high “Cholesterin” (translates as simply “cholesterol”. Not sure if this is total cholesterol, because it’s higher than my HDL+LDL) value, but I’m only 37 years old, with a BMI of 20.8, and my triglyceride levels are obviously good! (What may be of interest, is that my urine Ketone Bodies were measured at 80, which of course also got a *).
I’ve never had high cholesterol before. Does it make sense that the KETO diet is causing it? Should I stop? I am NOT loosing weight at the moment – that was never my goal. In fact I used to be underweight, and for the first time ever am now a healthy weight.
Thanks in advance for any help you can give me! I appreciate all the work you and Maria do for us all 🙂
Thank you so much for your quick reply! My CRP (assuming that’s “C-reaktives Protein) is 2.3 (normal 0-5), so that’s probably fine. Can’t figure out what the A1c is in German 😉 If total cholesterol is HDL+LDL, then mine is 298.40, which I assume is actually too high. So confusing!
Good to hear that people can have high cholesterol levels and still have a low calcium score run, though. Will try not to worry 🙂
With this lifestyle, over time, your CRP should come down. Low risk: CRP level of less than 1.0 milligrams per liter (mg/L).
Average risk: CRP level between 1.0 and 3.0 mg/L.
High risk: CRP level greater than 3.0 mg/L.
Ideally about 0.5
As for A1c, ideal is below 5.
Wonderful! Thanks for the info 🙂